
Stroke Rehabilitation for Athletes
Stroke Rehabilitation for Athletes needs equal parts neuroscience and smart strength work. Athletes recover faster when rehab builds skill, confidence, and fitness in a clear progression that links clinic to field.
What stroke rehabilitation should include
AHA and ASA guidelines recommend structured, goal driven programs that emphasize task specific practice, progressive exercise, and education across the continuum of care. These guidelines also outline when to add specialized options such as constraint induced movement therapy and how to manage dosing early after stroke. PubMed
Key pillars
- Task specific training to rebuild useful skills like sit to stand, stepping, reaching, and grasping. Reviews show benefits for functional outcomes compared with non task approaches. PubMedAOTA Research
- Strength training with gradual loading to treat hemiparesis and restore symmetry.
- Aerobic training to reverse low fitness and improve walking ability and quality of life. Recommended prescriptions commonly build from 20 to 40 minutes at 3 to 5 days per week after screening. PMCPubMed
- Dose awareness in the first 24 hours. AVERT research cautions against very early high dose upright activity. Shorter, more frequent bouts are safer at this stage. The LancetAmerican Academy of Neurology
Internal links for warm up and movement quality: start sessions with our Four Worlds Movement Framework and revisit core control with Core Stability at EvoFitLab.
Quick screen and red flags
- History of unilateral weakness, numbness, or coordination loss with confirmed stroke.
- Observe sit to stand, 10 meter walk, and single arm reach to guide first goals.
- Urgent referral if new or worsening neurologic signs appear.
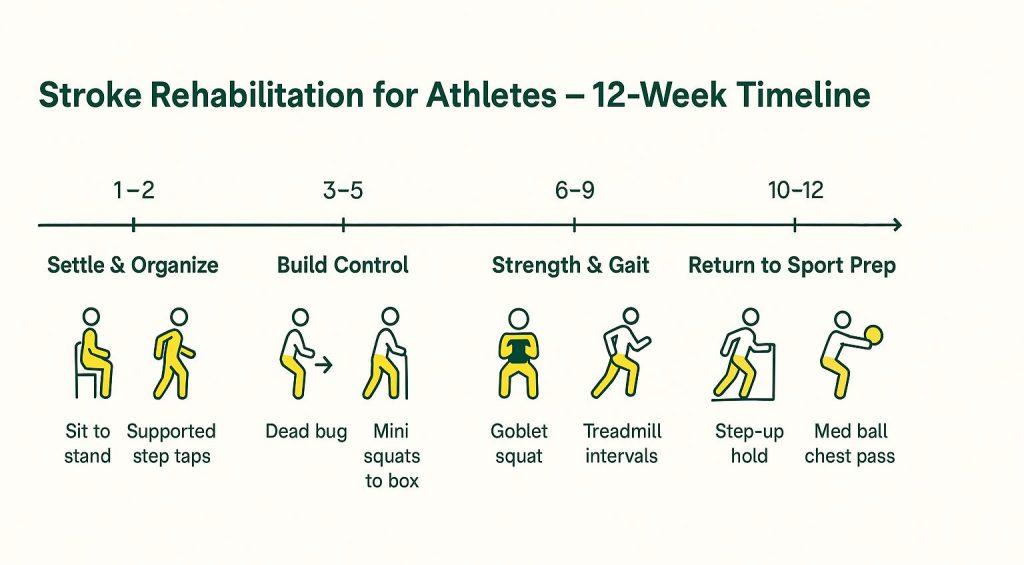
12-week plan at a glance
Progress only when pain is controlled, vitals stay stable, and movement quality holds. Each phase lists session ideas. Pick two or three per session.
| Phase | Weeks | Main goals | Sample work |
|---|---|---|---|
| 1. Settle and organize | 1–2 | Protect, educate, light practice | Sit to stand 3×6, supported step taps 3×20 m total, supported reach and grasp practice 5 min, easy cycling or treadmill 10–15 min |
| 2. Build control | 3–5 | Trunk and hip control, arm use | Dead bug 3×8, side bridge 3×15–20 s, mini squats to box 3×8, supported farmer carry 4×20 m, reach to targets 5 min |
| 3. Strength and gait | 6–9 | Symmetry and speed | Goblet squat 3×6–8, split squat 3×6 each, hip hinge to dowel 3×8, treadmill intervals 6×1 min easy or moderate, overground cadence drills |
| 4. Return to sport prep | 10–12 | Direction change, carry and lift, confidence | Step up and hold 3×6 each, med ball chest pass 3×6, low hurdle marching and lateral steps, circuit of carry, push, pull for 10–15 min |
Why task specific practice? Cochrane and related summaries support repetitive, meaningful, task oriented methods to improve activities of daily living and mobility after stroke. Cochrane LibraryAOTA Research
Aerobic and strength prescriptions
- Aerobic after screening: begin at 20 minutes total and progress toward 30 to 40 minutes, 3 to 5 days per week at 40 to 50 percent of heart rate reserve then build toward 60 to 80 percent as tolerated. Benefits include aerobic capacity and walking gains. PubMed
- Strength two or three days weekly: sit to stand, squats to a box, RDL patterning, row and press variations. Use loads that allow crisp technique.
- Upper limb candidates may trial modified constraint induced movement therapy blocks to boost affected arm use in daily tasks. CochranePMC
Internal link for power work later in rehab: when ready for faster intent, see Rate of Force Development Training. For long term planning, review our Fitness Periodization Guide. Explore more resources in the EvoFitLab blog hub.
Safety and monitoring
- Check resting blood pressure and heart rate before sessions.
- Keep RPE between easy and moderate in early phases.
- Video basic tasks to audit alignment and progress.
- Respect fatigue. If technique degrades, trim volume.
When to involve specialists
Follow medical advice on imaging, medications, or injections. AHA and ASA guidance remains the reference for multidisciplinary care across acute, subacute, and chronic stages. AHA Journals
Conclusion
Stroke Rehabilitation for Athletes works best when practice looks like life and training builds fitness step by step. Use this plan to rebuild control, strength, and confidence over twelve weeks, then keep a small weekly dose of skill, strength, and cardio to stay resilient.
Written by Gerard Nicholas, CSCS










